
Contrast enhanced ultrasound in pediatric patients
March 09, 2018
By Dr. Beth McCarville
At St. Jude Children’s Research Hospital, we recently treated a 10-year-old girl with recurrent acute myelogenous leukemia who had undergone a bone marrow transplant.
Shortly after the transplant, she developed hepatic-veno-occlusive disease, a condition in which some of the small veins in the liver are obstructed.
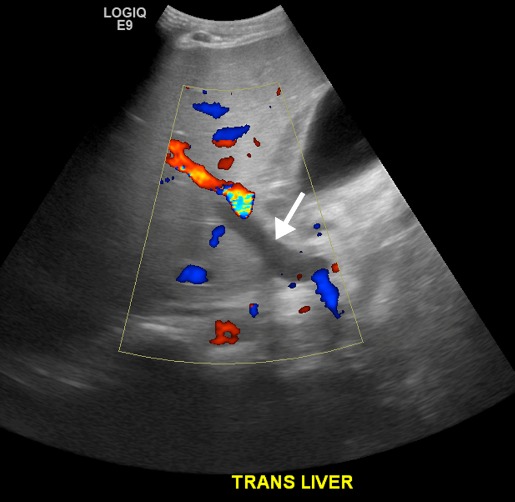
She was treated with blood thinners, yet her liver function worsened. We performed color Doppler and 2-D spectral Doppler ultrasound of her liver to assess the blood flow. The examination revealed an absence of flow in the main portal vein, but it was unclear whether this was due to portal vein thrombosis (a blockage or narrowing of the portal vein by a blood clot) or venous stasis (a risk factor for forming blood clots in veins). Portal vein thrombosis would require delivery of tissue plasminogen activator (TPA) directly into the portal vein while venous stasis could be managed conservatively.
In this patient, intravascular TPA carried numerous associated risks and therefore, it was crucial to confirm the presence of thrombus. Because the patient had undergone myeloablation in preparation for bone marrow transplantation, she was thrombocytopenic, coagulopathic and at a high risk of bleeding from invasive procedures such as required for TPA administration.
Also, her transplant had induced renal insufficiency. Because of this, she was not a good candidate for any imaging procedure requiring the use of an iodinated intravenous contrast agent due to the potential for toxicity in the kidneys. Moreover, because she was in critical condition, she was not a good candidate for transport to the imaging department for MR angiography.

She was, however, an ideal candidate for contrast enhanced ultrasound (CEUS). Ultrasound contrast agents are not metabolized by the kidneys, so they can be safely administered to patients with renal insufficiency. Ultrasound is also a portable modality that can be easily transported outside of the radiology department.
We performed a CEUS exam at the patient’s bedside which clearly demonstrated reversal of flow in the main portal vein. In this case, CEUS answered a crucial clinical question while eliminating the need for a risky invasive procedure, avoided the potential nephrotoxicity from iodinated contrast administration, avoided exposing the patient to additional ionizing radiation and avoided transporting a critically ill patient out of the intensive care unit.
Approximately 30 million people in the U.S. have some form of liver disease. However, its symptoms can be vague and easily confused with other health complications, making it difficult to diagnose.
In April 2016, the FDA approved the use of contrast agent for liver lesion characterization in adult and pediatric patients, offering clinicians a fast way of confidently detecting problems in a patient’s liver, using non-ionizing radiation.
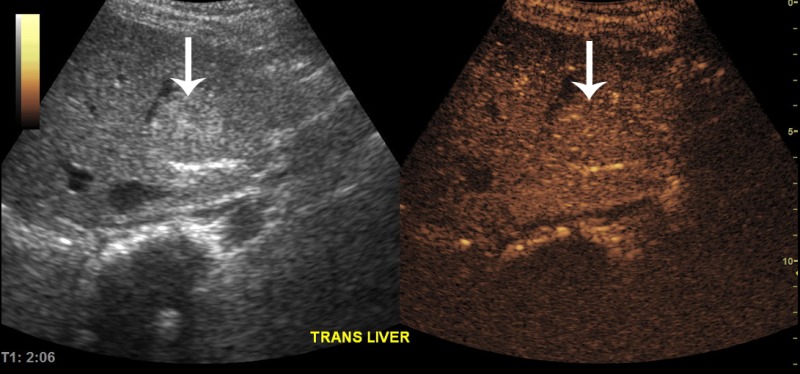
Our main clinical indication for contrast enhanced ultrasound (CEUS) is to characterize focal liver lesions. Focal liver lesions occur in about 17 percent of children after cancer therapy. When such lesions arise, it is crucial to determine whether they are benign or represent metastatic disease. Before utilizing CEUS at our institution, such patients would undergo additional imaging (often MRI which can require sedation of young patients) or early imaging follow-up to determine the growth rate of the lesion. This approach resulted in added time, cost and anxiety in the patient’s management.

Now these patients undergo CEUS on the same day or the next day after the original imaging exam that discovered the focal liver lesion. This approach is quick, low-cost, uses non-ionizing radiation and is sedation-free. It provides immediate clinical images, which enables physicians to give feedback to the patient, their family and treating physician.
I believe the role of CEUS in pediatric oncology will increase. There are a wide variety of potential applications. In addition to being low-cost and sedation-free, it has the added benefit of being portable. This is an important attribute in our institution because patients needing imaging studies may be too ill to come to the radiology department. The system can be easily transported to their bedside. Children are naturally in motion, so it’s important to be able to capture clear images quickly.
With the introduction of targeted therapies into cancer clinical trials, there is a growing need for functional and metabolic imaging methods that go beyond a simple measurement of tumor size. Dynamic, quantitative contrast enhanced ultrasound may provide a method of assessing tumor blood flow which, in turn, may reflect or predict response to therapy.  This, however, needs to be validated in clinical trials.
This, however, needs to be validated in clinical trials.
About the author: Dr. Beth McCarville is the chief of the Body Imaging Section at St. Jude Children’s Research Hospital.
At St. Jude Children’s Research Hospital, we recently treated a 10-year-old girl with recurrent acute myelogenous leukemia who had undergone a bone marrow transplant.
Shortly after the transplant, she developed hepatic-veno-occlusive disease, a condition in which some of the small veins in the liver are obstructed.
She was treated with blood thinners, yet her liver function worsened. We performed color Doppler and 2-D spectral Doppler ultrasound of her liver to assess the blood flow. The examination revealed an absence of flow in the main portal vein, but it was unclear whether this was due to portal vein thrombosis (a blockage or narrowing of the portal vein by a blood clot) or venous stasis (a risk factor for forming blood clots in veins). Portal vein thrombosis would require delivery of tissue plasminogen activator (TPA) directly into the portal vein while venous stasis could be managed conservatively.
In this patient, intravascular TPA carried numerous associated risks and therefore, it was crucial to confirm the presence of thrombus. Because the patient had undergone myeloablation in preparation for bone marrow transplantation, she was thrombocytopenic, coagulopathic and at a high risk of bleeding from invasive procedures such as required for TPA administration.
Also, her transplant had induced renal insufficiency. Because of this, she was not a good candidate for any imaging procedure requiring the use of an iodinated intravenous contrast agent due to the potential for toxicity in the kidneys. Moreover, because she was in critical condition, she was not a good candidate for transport to the imaging department for MR angiography.
She was, however, an ideal candidate for contrast enhanced ultrasound (CEUS). Ultrasound contrast agents are not metabolized by the kidneys, so they can be safely administered to patients with renal insufficiency. Ultrasound is also a portable modality that can be easily transported outside of the radiology department.
We performed a CEUS exam at the patient’s bedside which clearly demonstrated reversal of flow in the main portal vein. In this case, CEUS answered a crucial clinical question while eliminating the need for a risky invasive procedure, avoided the potential nephrotoxicity from iodinated contrast administration, avoided exposing the patient to additional ionizing radiation and avoided transporting a critically ill patient out of the intensive care unit.
Approximately 30 million people in the U.S. have some form of liver disease. However, its symptoms can be vague and easily confused with other health complications, making it difficult to diagnose.
In April 2016, the FDA approved the use of contrast agent for liver lesion characterization in adult and pediatric patients, offering clinicians a fast way of confidently detecting problems in a patient’s liver, using non-ionizing radiation.
Our main clinical indication for contrast enhanced ultrasound (CEUS) is to characterize focal liver lesions. Focal liver lesions occur in about 17 percent of children after cancer therapy. When such lesions arise, it is crucial to determine whether they are benign or represent metastatic disease. Before utilizing CEUS at our institution, such patients would undergo additional imaging (often MRI which can require sedation of young patients) or early imaging follow-up to determine the growth rate of the lesion. This approach resulted in added time, cost and anxiety in the patient’s management.
Now these patients undergo CEUS on the same day or the next day after the original imaging exam that discovered the focal liver lesion. This approach is quick, low-cost, uses non-ionizing radiation and is sedation-free. It provides immediate clinical images, which enables physicians to give feedback to the patient, their family and treating physician.
I believe the role of CEUS in pediatric oncology will increase. There are a wide variety of potential applications. In addition to being low-cost and sedation-free, it has the added benefit of being portable. This is an important attribute in our institution because patients needing imaging studies may be too ill to come to the radiology department. The system can be easily transported to their bedside. Children are naturally in motion, so it’s important to be able to capture clear images quickly.
With the introduction of targeted therapies into cancer clinical trials, there is a growing need for functional and metabolic imaging methods that go beyond a simple measurement of tumor size. Dynamic, quantitative contrast enhanced ultrasound may provide a method of assessing tumor blood flow which, in turn, may reflect or predict response to therapy.

Dr. Beth McCarville
About the author: Dr. Beth McCarville is the chief of the Body Imaging Section at St. Jude Children’s Research Hospital.