
Dr. Nick van Terheyden
The value of clinical documentation
March 20, 2011
This report originally appeared in the March 2011 issue of DOTmed Business News
By Dr. Nick van Terheyden
Clinical documentation, while continuing to be the lifeblood of medicine remains a burden to capture, and oftentimes is associated with physician dissatisfaction and escalating costs.
Overcoming these barriers and bringing the documentation process into the 21st century is a key element in any facility’s strategy to deliver high quality patient care at lower costs. As part of this, there is a widely accepted premise that a core component to improving health care quality requires the implementation of an electronic medical record, a system that also happens to be the prime force behind clinical documentation change and improvement.
Today, the adoption rate of EMRs remains disappointingly low with only 7 – 13 percent of providers using a system today; this is based on the HIMSS Analytics database and its analysis of EMR adoption. As part of this analysis, it was determined that physician resistance to EMRs ranks as one of the top three reasons for perceived barriers to adoption.
To further emphasize this point, findings from a recent survey (http://www.nuance.com/healthcare/ehr-meaningful-use-study/) conducted by Nuance, which explored the physician perception of adopting EMRs found that there is a clear sense of increased burden of documentation required to interact with an EMR. The results of the survey also confirmed that physician resistance is linked to challenges associated with utilizing the keyboard and mouse for EMR data input. Another leading obstacle for clinicians is their fear that through using the EMR, they won’t easily be able to capture the patient’s unique story – due to an increased need to type details versus being able to dictate them.
The truth remains, that the most efficient means to capture clinical information is via traditional dictation. While traditional dictation, when supported by a medical transcriptionist who listens to what a clinician dictates and types the medical record may support the clinician in a workflow in which they feel comfortable, it is a costly process. Additionally, the information generated as part of this traditional workflow is in a format that is unreadable by an EMR system. Information that is captured in an EMR must contain discrete data that is semantically interoperable with EMRs versus long clinician narratives.
Today, there is efficient and cost-effective ways to support the clinical documentation process. Because many clinicians struggle with documenting via the keyboard, however, let them dictate! But do so in a better way than traditional workflow, speech-enable it.

Getting from A to B (traditional transcription supported clinical documentation to clinicians using an EMR system with no other support) is not easy. Above the line of disruption, shown at point A, there is no change required in physician behavior, below the line, shown at point B, physicians must adapt to new solutions and change their working practices. While there are benefits to these changes, the additional effort and skills required of busy clinicians can be overwhelming. EMR workflow also tends to interrupt the diagnostic process by requiring the clinician to focus on the system (the keyboard, screen and mouse) rather than focusing on the patient. This can lead to patient and clinician dissatisfaction.
There are many reasons health care organizations should consider speech recognition, particularly if they are looking for ways to ease the burden of an EMR implementation. Speech recognition relieves physicians of the need to point and click through structured EMR templates to convey a complicated patient narrative. With EMRs, it has really transitioned to being a fundamental enabler to the system.
The first step toward achieving physician buy-in is to understand your choices and their associated pros and cons. There are two types of speech-recognition technology:
• Backend: A physician dictates into a digital dictation system that records an audio file. The file is then converted to a centralized system where it is recognized and subsequently edited by a transcriptionist.
• Frontend: A physician dictates into a speech-recognition engine in which words are recognized and displayed immediately after they are spoken. The dictator is responsible for editing and signing off on the document.
As shown in figure 1, the challenge of clinical documentation can be addressed by marrying tailored technologies with clinicians’ preferred workflows. At this day and age, it is unreasonable to have clinicians fully reliant on medical transcriptionists who perform in the traditional way (typing documents from scratch); the simple reason being cost and non-compliance with EMRs.
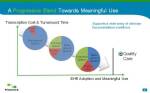
It is clear based on surveys and experience in the busy clinical setting that to achieve a high level of EMR penetration a blend of solutions is necessary for capturing and entering data. Taking this approach will lead physicians from the current status of clinical documentation capture (traditional dictation) to transcription with background speech recognition then in turn to the increasing use of front-end technology combined with other innovations for data capture including the mouse and keyboard.
Proven technology is offering a bridge over the line of disruption by allowing physicians to document their clinical encounter without the frustration of solely interacting with a time consuming point-and-click interface. Regardless of the method provided, the key to success in any clinical setting is providing clinicians with choices. In a regular clinic setting the physician may elect to use the front-end tools to capture the patient history and impression but as the day progresses and the workload increases the option to move to a background speech solution is available at any time. With choice always available to the clinicians in different clinical settings, resistance disappears as physicians feel empowered to make their own choice that suits their individual circumstances and patient load.
In every scenario, figuring out the capture component of the equation is first and foremost. Moving forward, however, we will see many health care organizations leveraging the power of Clinical Language Understanding (CLU), a technology that can extract clinically relevant data points from a clinician’s narrative and auto populate an EMR system. CLU, which has been referenced as the driving force behind Medical Intelligence will allow physicians to fully document patient encounters and medical decision-making details in their own words via speech-recognized dictation, while simultaneously extracting key clinical data, including: patient complaints, physician-assessed diagnoses, medication and procedural treatments, and health-related habits.
Imagine the value of a system, combining speech recognition and CLU, that not only recognizes what a physician is saying, but understands the meaning so that critical and relevant information can be automatically extracted, encoded into standardized medical vocabularies and shared with caregivers across the ecosystem of clinical systems.
Dr. Nick van Terheyden is the chief medical information officer for Nuance Communications. He brings a distinctive blend of medical practitioner and business strategist, to the realm of healthcare technology. Dr. van Terheyden is a pioneering creator in the evolution of health care technology and has worked as a business leader in one of the first speech recognition Internet companies.
By Dr. Nick van Terheyden
Clinical documentation, while continuing to be the lifeblood of medicine remains a burden to capture, and oftentimes is associated with physician dissatisfaction and escalating costs.
Overcoming these barriers and bringing the documentation process into the 21st century is a key element in any facility’s strategy to deliver high quality patient care at lower costs. As part of this, there is a widely accepted premise that a core component to improving health care quality requires the implementation of an electronic medical record, a system that also happens to be the prime force behind clinical documentation change and improvement.
Today, the adoption rate of EMRs remains disappointingly low with only 7 – 13 percent of providers using a system today; this is based on the HIMSS Analytics database and its analysis of EMR adoption. As part of this analysis, it was determined that physician resistance to EMRs ranks as one of the top three reasons for perceived barriers to adoption.
To further emphasize this point, findings from a recent survey (http://www.nuance.com/healthcare/ehr-meaningful-use-study/) conducted by Nuance, which explored the physician perception of adopting EMRs found that there is a clear sense of increased burden of documentation required to interact with an EMR. The results of the survey also confirmed that physician resistance is linked to challenges associated with utilizing the keyboard and mouse for EMR data input. Another leading obstacle for clinicians is their fear that through using the EMR, they won’t easily be able to capture the patient’s unique story – due to an increased need to type details versus being able to dictate them.
The truth remains, that the most efficient means to capture clinical information is via traditional dictation. While traditional dictation, when supported by a medical transcriptionist who listens to what a clinician dictates and types the medical record may support the clinician in a workflow in which they feel comfortable, it is a costly process. Additionally, the information generated as part of this traditional workflow is in a format that is unreadable by an EMR system. Information that is captured in an EMR must contain discrete data that is semantically interoperable with EMRs versus long clinician narratives.
Today, there is efficient and cost-effective ways to support the clinical documentation process. Because many clinicians struggle with documenting via the keyboard, however, let them dictate! But do so in a better way than traditional workflow, speech-enable it.
Getting from A to B (traditional transcription supported clinical documentation to clinicians using an EMR system with no other support) is not easy. Above the line of disruption, shown at point A, there is no change required in physician behavior, below the line, shown at point B, physicians must adapt to new solutions and change their working practices. While there are benefits to these changes, the additional effort and skills required of busy clinicians can be overwhelming. EMR workflow also tends to interrupt the diagnostic process by requiring the clinician to focus on the system (the keyboard, screen and mouse) rather than focusing on the patient. This can lead to patient and clinician dissatisfaction.
There are many reasons health care organizations should consider speech recognition, particularly if they are looking for ways to ease the burden of an EMR implementation. Speech recognition relieves physicians of the need to point and click through structured EMR templates to convey a complicated patient narrative. With EMRs, it has really transitioned to being a fundamental enabler to the system.
The first step toward achieving physician buy-in is to understand your choices and their associated pros and cons. There are two types of speech-recognition technology:
• Backend: A physician dictates into a digital dictation system that records an audio file. The file is then converted to a centralized system where it is recognized and subsequently edited by a transcriptionist.
• Frontend: A physician dictates into a speech-recognition engine in which words are recognized and displayed immediately after they are spoken. The dictator is responsible for editing and signing off on the document.
As shown in figure 1, the challenge of clinical documentation can be addressed by marrying tailored technologies with clinicians’ preferred workflows. At this day and age, it is unreasonable to have clinicians fully reliant on medical transcriptionists who perform in the traditional way (typing documents from scratch); the simple reason being cost and non-compliance with EMRs.
It is clear based on surveys and experience in the busy clinical setting that to achieve a high level of EMR penetration a blend of solutions is necessary for capturing and entering data. Taking this approach will lead physicians from the current status of clinical documentation capture (traditional dictation) to transcription with background speech recognition then in turn to the increasing use of front-end technology combined with other innovations for data capture including the mouse and keyboard.
Proven technology is offering a bridge over the line of disruption by allowing physicians to document their clinical encounter without the frustration of solely interacting with a time consuming point-and-click interface. Regardless of the method provided, the key to success in any clinical setting is providing clinicians with choices. In a regular clinic setting the physician may elect to use the front-end tools to capture the patient history and impression but as the day progresses and the workload increases the option to move to a background speech solution is available at any time. With choice always available to the clinicians in different clinical settings, resistance disappears as physicians feel empowered to make their own choice that suits their individual circumstances and patient load.
In every scenario, figuring out the capture component of the equation is first and foremost. Moving forward, however, we will see many health care organizations leveraging the power of Clinical Language Understanding (CLU), a technology that can extract clinically relevant data points from a clinician’s narrative and auto populate an EMR system. CLU, which has been referenced as the driving force behind Medical Intelligence will allow physicians to fully document patient encounters and medical decision-making details in their own words via speech-recognized dictation, while simultaneously extracting key clinical data, including: patient complaints, physician-assessed diagnoses, medication and procedural treatments, and health-related habits.
Imagine the value of a system, combining speech recognition and CLU, that not only recognizes what a physician is saying, but understands the meaning so that critical and relevant information can be automatically extracted, encoded into standardized medical vocabularies and shared with caregivers across the ecosystem of clinical systems.
Dr. Nick van Terheyden is the chief medical information officer for Nuance Communications. He brings a distinctive blend of medical practitioner and business strategist, to the realm of healthcare technology. Dr. van Terheyden is a pioneering creator in the evolution of health care technology and has worked as a business leader in one of the first speech recognition Internet companies.